
Isn’t “auto” always good? Automatic parking assistant in your car, auto focus of your camera, auto heating system for your home – it just makes life so much easier! When it comes to the immune system: definitely not. In this case “auto” means “against itself”, implicating that the immune system fails to distinguish between self and foreign and damages the body’s own tissues. More than 100 autoimmune diseases such as diabetes type 1, rheumatoid arthritis, vitiligo, and systemic lupus erythematosus are nowadays known (https://www.aarda.org). All these diseases have in common, that they are induced by self-reactive T cells, autoimmune antibodies, or deposition of immune complexes in tissues (Janeway et al., 2001). Moreover, they are chronic and incurable. In some cases, drugs can be given to relieve pain and prevent worsening of the symptoms. However, several autoimmune diseases (so far) cannot be treated at all. Did you know that groceries and health food shops – not pharmacies – for some patients are indispensable for relieving their symptoms? For coeliac disease, specific food rather than drugs helps patients to rehabilitate: All the gluten-free products in the shelves are not merely consumed by people who follow up-to-date dietary trends or for any other reasons omit gluten from their diet. In the first place, they are the only source for coeliac disease patients to eat bread, pizza, cookies, or cake. But what exactly is coeliac disease and why do patients need to omit gluten from their diet?
Mysterious “wheat factor” – the trigger for coeliac disease
Already in the first century AD the Greek physician Aretaeus the Cappadocian described symptoms of adult patients suffering from chronic illness with ineffective digestion and assimilation of food as “the coeliac affection” (Greek: koiliakós – abdominal) (Dowd and Walker-Smith, 1974). In 1888, the English physician and paediatrician Samuel Gee seized this term for his patients that suffered from a condition that he identified as a “chronic indigestion” affecting people of all ages. At that time point it was not uncommon, that coeliac disease patients died due to a malnutrition. Thus, Gee stated that “if the patient can be cured at all, it must be by means of diet” (Dowd and Walker-Smith, 1974). Finally, Willem-Karel Dicke, a Dutch paediatrician, identified a “factor” of wheat as the trigger for the autoimmune response in coeliac disease patients in the early 1950s.

(image from colourbox.com/ Gelpi)
In his initial studies, Dicke could exclude wheat starch being harmful when consumed by patients. Subsequent studies of different fractions of wheat then identified “gluten” as the harmful substance (Yan and Holt, 2009). Gluten (Latin: gluten – glue) comprises a protein class of prolamins and gliadins which are rich in proline and glutamine. The gluten proteins found in the grains of the Triticeae tribe such as wheat, rye, spelt, triticale, kamut, emmer, einkorn, and green spelt are harmful for coeliac disease patients. Flours of these grains are frequently used by the food industry, since their prolamins and gliadins give both viscous and elastic properties to dough making this “two-component glue” ideal for bread baking (Wieser, 2007). But gluten is not only contained in food products, it is also found as an additive in cosmetics and medicine.
These Triticeae gluten proteins are harmful for coeliac disease patients as they – when being orally taken up – can evoke intestinal and extra-intestinal symptoms such as diarrhoea, weight loss, nutrient deficiencies, osteoporosis, fatigue, or peripheral neuropathy. In affected subjects, ingested gluten proteins can enter and cross the intestinal epithelial layer by an unknown mechanism, where they are modified by the tissue-resident transglutaminase (tTG): tTG deaminates gliadin, converting glutamine residues to glutamic acid, which is thought to favour the protein’s binding to the human leukocyte antigen (HLA)-DQ2 or -DQ8 on antigen-presenting cells (Ciccocioppo et al., 2005). CD4+ T cells recognize these gliadin epitopes, induce the release of pro-inflammatory cytokines, and evoke an infiltration of cytotoxic T cells. Moreover, CD4+ T cells stimulate B cells to produce anti-gliadin and anti-tTG antibodies (Ciccocioppo et al., 2005). Together, these immune reactions induce mucosal damage and villous atrophy in the small intestine.
Interestingly, about 40% of the healthy Western population carries the genetic predisposition for coeliac disease and express HLA-DQ2 and/or HLA-DQ8. However, the mechanisms underlying coeliac disease development in 1% of the population is still unknown (Dieli-Crimi R et al., 2015).
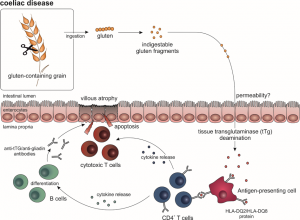
(figure by M. Woeste)
Going gluten-free – The devil is in the details
Now, as you know what gluten is and which grains contain it, let’s go gluten-free! I mean, not really, but as a thought experiment. Level 1: Buy some gluten-free bread or cereals for breakfast. Level 2: Lunch time: Go to the canteen and hope they offer some gluten-free meal or otherwise prepare something at home the day before. Level 3: You’re invited to a birthday party at the weekend? Perfect! That’s the best opportunity to test your gluten-free “strictness”. Let’s see if you can finish the levels or stumble into a pitfall:

(image from colourbox.com)
Level 1: You are usually buying your bread at the bakery? From now on refrain from buying bread there, since they don’t offer gluten-free products – if they do so, production of gluten-containing and gluten-free food is probably performed in the same factory, making products not suitable for coeliac disease patients due to cross-contamination with gluten. So, better go to the grocery store, since most of them nowadays offer gluten-free products. But: The assortment is small, so, if you don’t like to stick to one sort of bread or cereals for months or years, do “grocery hopping”. Info: Costs for gluten-free cereal products and sweets are nearly four times higher than for regular products (German Coeliac Society (Deutsche Zöliakie Gesellschaft): Ergebnisse der DZG Mehrkostenstudie, 2015).
Level 2: Lunch time: Although, it’s already 20 people waiting in the line behind you, try to focus the canteen staff on the following question: “Does this meal contain any gluten?” If the answer is “No, there’s no glutamate in it”, explain them that you meant gluten, not glutamate. At this point, it’s better to ask the cook for the meals’ ingredients. Luckily (or unfortunately?), you are really hungry – this will help you to blind out that the waiting line behind you is growing exponentially. After having spoken to the cook: You are lucky! Today the canteen offers some meal suitable for you: rice, vegetables, and steak! Points deduction: You cannot take the sauce, since it contains a gluten-based sauce thickener. Before coming to level 3, you might need to repeat step 2 several times unless you don’t start to cook at home with products you know are gluten-free.
Level 3: It’s Friday – finally weekend! You have already bought a present for your friend’s birthday, now it’s time to think about some gluten-free snacks and drinks you can bring. Lettuce and vegetables are naturally gluten-free, thus, preparing a salad is the easiest option. You used to be a beer drinker? Maybe, you should refrain from drinking beer, because 1. normal beer contains gluten and 2. a crate of gluten-free beer costs nearly 40 €.

(image from colourbox.com/ Panachai Cherdchucheep)
Could you imagine, being on a life-long diet like this? Unfortunately, coeliac disease patients need to do so to evade their bodies’ autoimmune response. Already 20 ppm of gluten (20 mg per kg) can have a deleterious effect for the patients. They are only allowed to eat naturally gluten-free foods (luckily, unprocessed meat, vegetables, and fruits are gluten-free) or special gluten-free products that contain less than 20 ppm of gluten (Bascuñán et al., 2017). Reading listed ingredients and keeping potential gluten contaminations in mind, especially when going out for dinner, is part of their every-day life.
Is there any therapy in sight? For most patients, omitting gluten from their diet already recovers their symptoms, thus, additional treatment diminishing the immune response is not needed. However, some patients not sufficiently recover upon a gluten-free diet and might need additional therapies to antagonize the immune response. Potential targets currently studied are inhibitors for the tissue transglutaminase, peptidases that can degrade gluten proteins, inhibitors for HLA-DQ presentation of gluten peptides to T cells, interleukin treatment to antagonise the evoked immune response, or drugs that prevent the gluten-induced damage of tight junctions in the intestinal epithelium (Govind, 2014).
Taken together, there is still a lot to learn about coeliac disease, especially its causes. Interesting aspects are covered by the research of the gastroenterologist Prof. Dr. Dr. Schuppan, head of the Institute of Translational Immunology at the University Mainz and professor at Harvard Medical School in Boston. Moreover, the German Coeliac Society offers many information (e.g. diagnosis, gluten-free diet) and supports patients suffering from coeliac disease.
References and Sources:
https://www.aarda.org. American Autoimmune Related Diseases Association
https://www.dzg-online.de
https://www.dzg-online.de/files/2015_2_ergebnisse_mehrkostenstudie.pdf. Mehrkosten der gluten-freien Ernährung bei Zöliakie – Ergebnisse der DZG Mehrkostenstudie.
Bascuñán K.A., Vespa M.C., Araya M., Celiac disease: understanding the gluten-free diet. Eur J Nutr. 2017; 56(2):449-459.
Ciccocioppo R., Di Sabatino A, and Corazza G.R., The immune recognition of gluten in coeliac disease. Clin Exp Immunol. 2005; 140(3): 408–416.
Dieli-Crimi R., Cénit M.C., Núñez C., The genetics of celiac disease: A comprehensive review of clinical implications. Journal of Autoimmunity. 2015: 64: 26-41
Dowd B. and Walker-Smith J., Samuel Gee, Aretaeus, and the coeliac affection. Br Med J. 1974; 2(5909): 45–47.
Janeway C.A., Jr, Travers P., Walport M., and Shlomchik M.J., Immunobiology, 5th edition. The Immune System in Health and Disease. Chapter 13. Autoimmunity and Transplantation. New York: Garland Science; 2001.
van Berge-Henegouwen G.P. and Mulder C.J., Pioneer in the gluten free diet: Willem-Karel Dicke 1905-1962, over 50 years of gluten free diet. Gut. 1993; 34(11): 1473-5.
Wieser H., Chemistry of gluten proteins. Food Microbiol. 2007; 24(2): 115-9.
Yan D. and Holt P.R., Willem Dicke. Brilliant Clinical Observer and Translational Investigator. Discoverer of the Toxic Cause of Celiac Disease. Clin Transl Sci. 2009; 2(6): 446–448.
Govind K.M., Current and Emerging Therapy for Celiac Disease. Front Med (Lausanne). 2014; 1: 6.
(featured image from colourbox.com)
Marina Woeste