
In the last years gender related topics in all different forms have often made it to the front page of newspapers. Most likely, we all have seen headlines about the gender pay gap, the #MeToo movement or the discussion about unisex public toilets. But what about gender and science? When searching for the key words gender and science most of the hits cover the topics gender gap, underrepresentation of women in leadership or the differences between typically female and male dominated scientific fields. But what about gender and immunity? What does science tell us about the impact of gender on our immune system?
This has become a hot topic, as evidence suggests a strong male bias in COVID-19 disease severity, with a 1.7 times higher risk of death1. And we immunologists have some catching up to do here. Among ten biological disciplines, immunology ranks the lowest in terms of reporting the sex of animal or human subjects2. So, what do we know about sex differences and immunity?
It has been shown that men have a higher risk of death from malignant cancer and a higher infection rate and disease burden for several infectious diseases including HIV. On the other hand, women are more likely to suffer from autoimmune diseases such as multiple sclerosis2.
So how do we explain these epidemiological differences?
What basic research says about gender and immunity

First of all, some definitions. Whereas the sex of an individual is defined by chromosomes, sex hormone levels and reproductive organs, the term gender includes behaviors and activities influenced by society and culture. And not only sex, but also gender influences our immune system. For example, stereotypical female and male activities can influence the exposure to microorganisms and health seeking behaviors which then affect the course of infection.
One major difference due to biological sex is the level of sex hormones, especially androgens such as testosterone, estrogen and progesterone. All of them have been shown to influence innate and adaptive immune responses. Whereas estrogen has mainly proinflammatory effects, testosterone is mostly considered as immunosuppressive2. For example androgen deficient men show higher concentrations of inflammatory cytokines when compared to men with normal testosterone levels. When they were supplemented with testosterone, proinflammatory cytokine levels such as TNF significantly decreased3. At our university in Bonn, it was shown that low serum testosterone levels correlated with disease severity in male psoriatic patients, a chronic inflammatory skin disease with autoimmune background4.
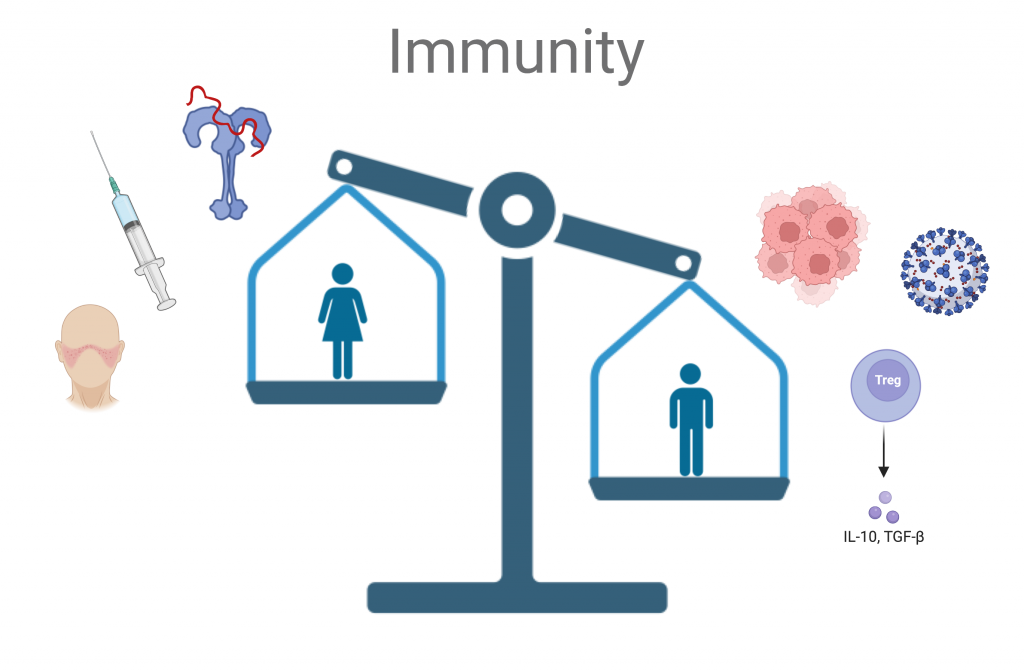
However, immune differences are not exclusively due to hormones. Genetically, many innate immune genes such as pattern recognition receptors (e.g. Toll-like receptor 7 and 8) and Interleukin receptors are expressed on the X chromosome. When escaping X inactivation this can lead to a higher expression in females as shown for TLR75. In the mouse model, it has been shown that gonadal female mice with an XY chromosome (transgenic SJL) demonstrated a lower susceptibility to lupus (autoimmune disease more prevalent in females) when compared to mice with an XX chromosome, proving the effect to be independent of differences in sex hormone levels6.
Why clinical scientists (should) care about gender and immunity
Considering these gender related differences in immune response, it might seem obvious that it should be standard practice in research to use male and female animals for in vivo experiments as well as male and female participants for clinical trials.
However, in 1977 the U.S. Food and Drug Administration (FDA) published guidelines advising that females of childbearing potential should be excluded from drug trials7. Even if back then it might have seemed like a reasonable way to protect potential unborn children, underrepresentation in clinical trials, results in a lack of knowledge such as potential sex specific adverse events or necessary dosage adjustments, resulting in an increased risk for women taking these drugs. For example, it was shown, that among the withdrawn drugs from U.S. market (1997-2000) 8 out of 10 drugs had greater adverse effects in females8. Even though we have made substantial progress over time including the FDA’s advice to include females in clinical trials in 19909, until today there are still far too many scientists who prefer to use male animals10.
But let us look at one example of male and female disparities in more detail. Checkpoint inhibitors have revolutionized the treatment of several cancer entities in advanced stages. Inhibition of “Immune-Checkpoints” such as cytotoxic T lymphocyte-associated protein 4 or programmed death 1 releases the “break” enabling the host immune system to fight the cancer. Several Meta-analyses reveal that both overall survival but also progression-free survival is higher in males compared to females receiving checkpoint inhibitors against several types of cancer such as melanoma and non-small-cell lung cancer11. In immune checkpoint inhibitor therapy, autoimmune-mediated complications, also known as immune-related adverse events are one of the most common serious side effects. Albeit existing broad knowledge about the role of dosage and type of checkpoint inhibitor and immune-related adverse events, little is known about differences between male and female patients12. Considering that autoimmune disease are more prevalent in women, a higher frequency and magnitude of immune-related adverse events seems likely and would merit further investigation.
But before this blog article turns into an actual scientific review I will stop here, hoping that I have convinced a few immunologists and immunologists to be, to always consider gender when publishing a paper so we can leave the worst ranked biological discipline in terms of reporting the sex of animal or human subjects behind us. After all gender influences much more than just COVID-19 disease severity.
Author: Maike Adamson
References:
1. Scully, E. P., Haverfield, J., L., U., Rebecca, Tannenbaum, C. & Klein, S. L. Considering how biological sex impacts immune responses and COVID-19 outcomes. 20, 442–447 (2020).
2. Klein, S. L. & Flanagan, K. L. Sex differences in immune responses. 16, 626–638 (2016).
3. Malkin, C. J. et al. The Effect of Testosterone Replacement on Endogenous Inflammatory Cytokines and Lipid Profiles in Hypogonadal Men. The Journal of Clinical Endocrinology & Metabolism 89, 3313–3318 (2004).
4. Allam, J.-P. et al. Low serum testosterone levels in male psoriasis patients correlate with disease severity. 29, 375 (2019).
5. Smith-Bouvier, D. L. et al. A role for sex chromosome complement in the female bias in autoimmune disease. Journal of Experimental Medicine 205, 1099–1108 (2008).
6. P, P. et al. Autoreactive B cell responses to RNA-related antigens due to TLR7 gene duplication. Science (2006).
7. General Considerations for the Clinical Evaluation of Drugs. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/general-considerations-clinical-evaluation-drugs.
8. Simon, V. Wanted: Women in Clinical Trials. Science 308, 1517–1517 (2005).
9. Pinn, V. W. The role of the NIH’s Office of Research on Women’s Health. Academic Medicine 69,.
10. Beery, A. K. & Zucker, I. Sex bias in neuroscience and biomedical research. Neuroscience & Biobehavioral Reviews 35, 565–572 (2011).
11. Wu, Y. et al. Correlation between sex and efficacy of immune checkpoint inhibitors (PD-1 and CTLA-4 inhibitors). International Journal of Cancer 143, 45–51 (2018).
12. Özdemir, B. C., Coukos, G. & Wagner, A. D. Immune-related adverse events of immune checkpoint inhibitors and the impact of sex—what we know and what we need to learn. Annals of Oncology 29, 1067 (2018).